Somewhere between "miracle therapy" and "expensive wood box," the truth about infrared saunas tends to get lost. If you've tried to research whether one is right for you, you've probably found equal parts breathless endorsement and flat-out dismissal, with very little in the middle.
That frustration is understandable. The wellness industry has a habit of overselling heat therapy as a cure for almost everything, while skeptics sometimes dismiss real, institution-backed findings along with the hype. Neither approach helps you make a smart decision.
Here's what's actually true: infrared saunas are not a scam. The Mayo Clinic and Cleveland Clinic both acknowledge real health benefits from their use, and published research in peer-reviewed journals supports specific applications ranging from cardiovascular health to chronic pain relief. At the same time, some of the boldest claims circulating online, particularly around detoxification and weight loss, are not well supported by the same body of evidence. The technology works, but it doesn't work equally well for everything people claim it does.
Whether that physiological response translates into meaningful health outcomes depends heavily on which condition you're asking about. The cardiovascular evidence is fairly solid. The pain relief data, particularly for conditions like rheumatoid arthritis, is promising. The mood and sleep connections have real biological pathways behind them. The detox claims, on the other hand, require a much more careful look.
The research from the Mayo Clinic, Cleveland Clinic, and peer-reviewed journals shows:
- How infrared heat affects your body and why that mechanism matters
- What the skin and hair evidence really shows, separate from cosmetic marketing
- How the pain relief data holds up across joint, nerve, and muscle conditions
- What the mood, sleep, and stress research looks like, and what's driving it
- Where the cardiovascular and blood pressure benefits are most clearly supported
- How to think about respiratory and immune claims, including what helps and what doesn't
- What "detox" actually means in this context, and which parts of that story hold up
- Which specific health conditions require the most careful evaluation before you start
- The honest numbers on calorie burn and weight management
- Whether format matters, specifically whether an infrared sauna blanket delivers comparable results to a full cabin
By the end, you'll have a clear, condition-by-condition picture you can actually use, whether you're deciding whether to buy, evaluating a gym membership that includes access, or trying to figure out whether your specific health concern is one where the evidence genuinely supports giving it a try.
General Health & Wellness Claims
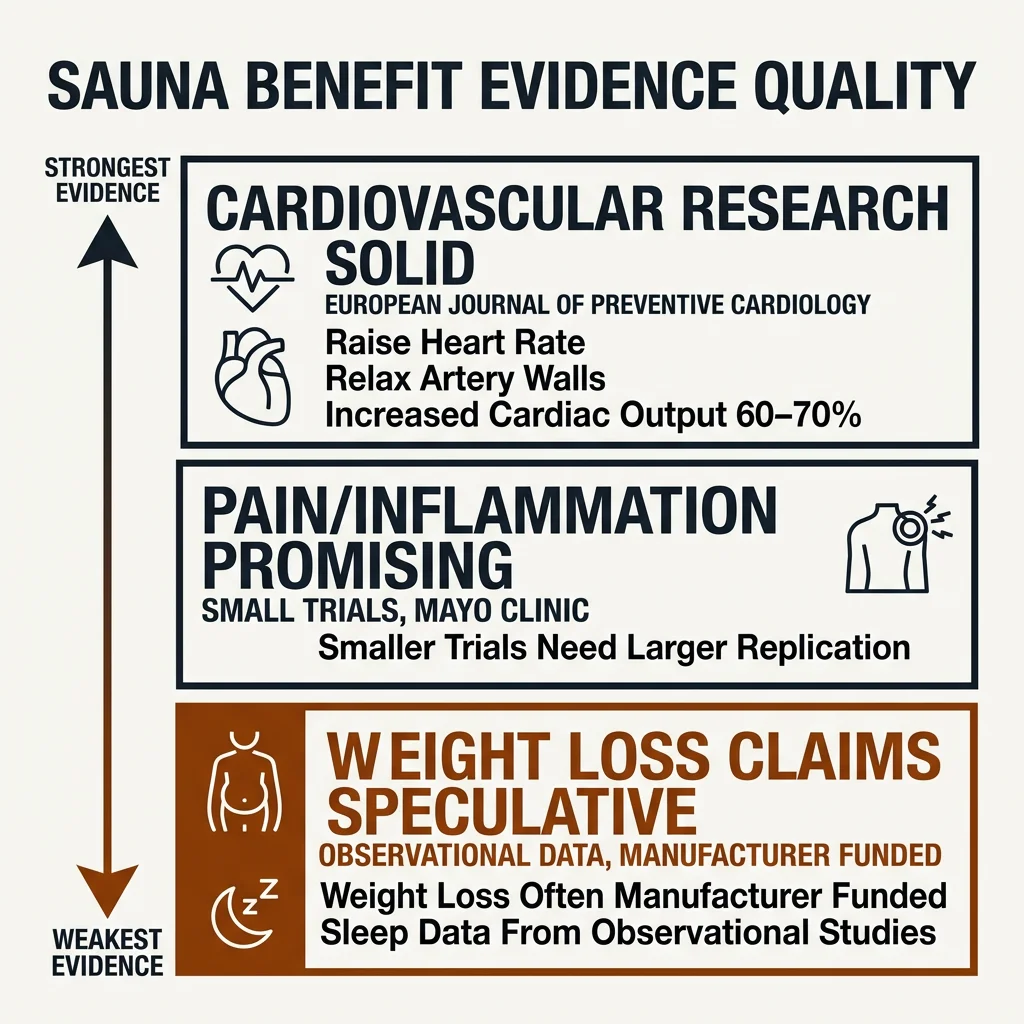
The research behind infrared saunas doesn't exist on a simple pass/fail axis. It spans a wide spectrum, from well-replicated clinical findings to early-stage trials to claims that rest almost entirely on manufacturer literature and wellness-site repetition. Understanding where a benefit falls on this spectrum helps evaluate claims based on evidence rather than skepticism.
What the research base actually looks like
The evidence quality spectrum runs from solid to speculative, and the distance between those ends is substantial. On the stronger end, cardiovascular research published in peer-reviewed journals, including the European Journal of Preventive Cardiology, documents measurable physiological changes: infrared heat raises heart rate, induces nitric oxide production, relaxes artery walls, and can increase cardiac output by 60-70%. These are documented biological responses with plausible mechanisms and independent publication records behind them.Further along the spectrum, you find pain and inflammation data that looks promising in smaller trials but still needs larger replications to be considered conclusive. The Mayo Clinic notes directly that studies on infrared sauna benefits are often small or in early stages, and that larger clinical trials remain needed for many conditions.
At the weakest end are claims that some independent researchers have flagged as needing more rigorous investigation. Weight loss, for instance, is a category where some of the existing studies have been funded by manufacturers, and the call for independent research is consistent across sources. The sleep data, while promising in places, primarily comes from observational studies and wellness-focused sources rather than controlled clinical research.
How infrared heat absorption works
The physiological chain begins with infrared heat absorption: infrared wavelengths penetrate skin tissue directly, raising core body temperature without requiring the surrounding air to reach extreme heat. Cleveland Clinic notes that infrared saunas typically bring core temperature to around 102°F (39°C). That thermal response drives the downstream effects, whether increased circulation, shifts in autonomic nervous system activity, or reductions in pro-inflammatory markers like IL-6 and TNF-α. The mechanism is real. The question, for any given condition, is how reliably that mechanism produces a clinically meaningful outcome.
Why the gap between mechanism and marketing exists
Because infrared heat absorption does produce measurable changes in cardiovascular response, inflammation markers, and autonomic nervous system activity, it's easy to extrapolate from "this works for condition X" to "this probably works for everything." That extrapolation is where credibility problems begin. The Cleveland Clinic and Mayo Clinic both acknowledge real benefits while being careful not to overstate them. What they've affirmed is real; what they've hedged is worth taking seriously.
Cardiovascular benefits clear all three questions reasonably well. Some pain relief and inflammation claims clear the first two but need larger replications. Weight loss claims often fall short on questions two and three, which is why the Mayo Clinic treats that area with particular caution.
Skin & Hair Health
A dermatologist reviewing most infrared sauna marketing copy would circle about half the claims in red pen. The skin benefits story is genuinely interesting, but it requires separating what the biology actually supports from what brands have extrapolated far beyond the evidence.
What infrared heat does to skin cells
The most credible skin-related mechanism starts with fibroblast activation. Fibroblasts are the cells responsible for producing collagen and elastin, the proteins that give skin its firmness and elasticity. When infrared heat reaches skin tissue, it activates these cells, prompting increased collagen and elastin production. Published research in peer-reviewed journals supports this chain of events, and the result is a modest improvement in skin firmness and texture over time.
The word "modest" matters here. The effects are supportive rather than dramatic, as Dermstore's dermatology coverage puts it. Infrared heat can help tighten skin, and the biological pathway explaining why is legitimate. What it cannot do is produce the kind of visible structural transformation that some brands suggest. Think of it as maintenance and mild improvement, not a clinical procedure.
Eczema and inflammatory skin conditions
This is where heat-triggered inflammatory response variability becomes important. Unlike cardiovascular effects, which tend to be fairly consistent across users, heat's effect on inflammatory skin conditions depends heavily on what triggers a given person's flares. Inflammation drives eczema, and infrared heat's documented effects on circulation may help reduce flares for some people. But Healthline notes that direct research on infrared saunas for eczema is limited, with most evidence coming from small studies or anecdotal reports.
Anyone with eczema should consult a dermatologist before adding infrared sessions to their routine, especially for moderate to severe cases. Infrared therapy is not a replacement for prescribed treatments; at best, it may be a useful complement for some people, depending on their specific triggers and history.
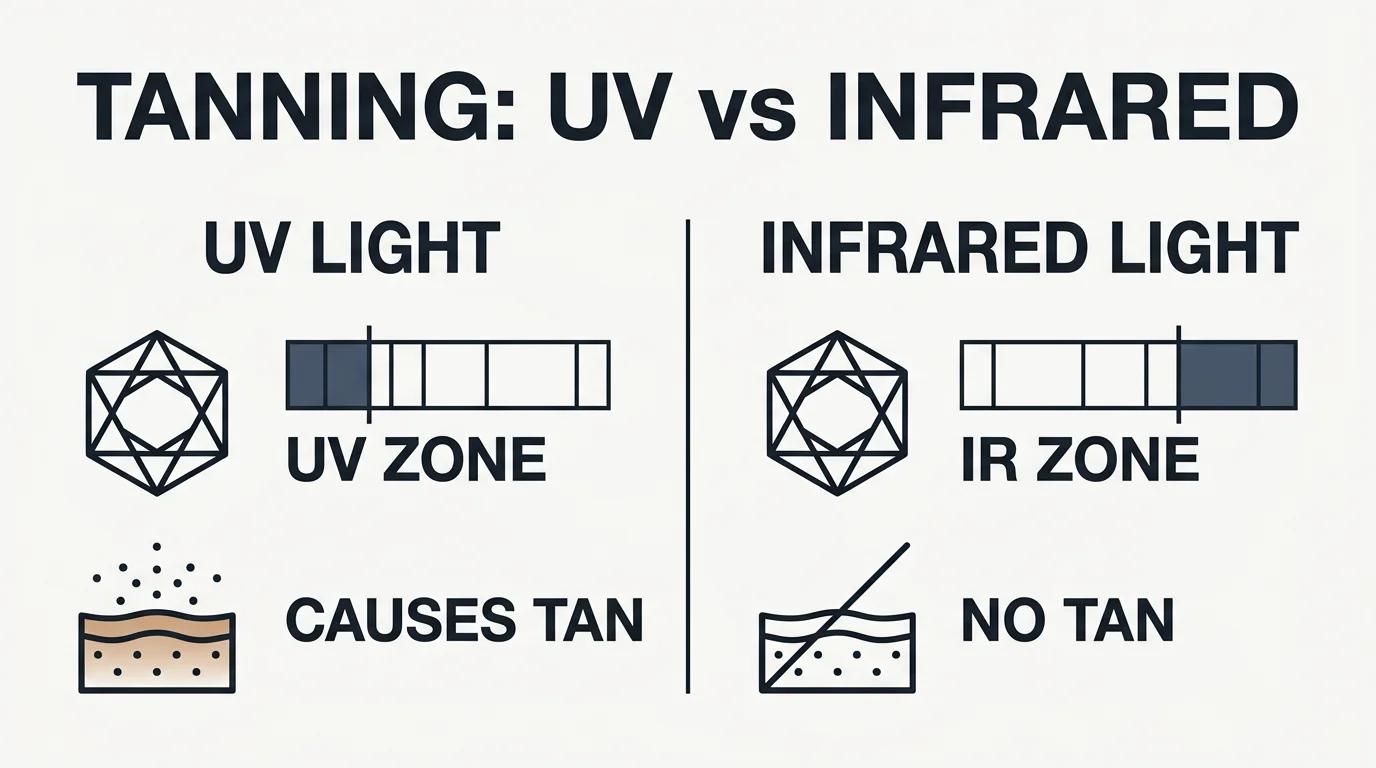
Why you won't tan, and the cancer question
Infrared light and ultraviolet light occupy entirely different parts of the electromagnetic spectrum. Tanning is driven by UV radiation triggering melanin production in skin cells. Infrared wavelengths don't trigger that response, which means no amount of sauna use produces a tan. No evidence links responsible infrared sauna use to skin cancer, according to Penn Derm Specialists, and the broader safety literature is consistent on this.
Pain Relief & Musculoskeletal Support
Infrared sauna research offers compelling insights into pain relief, though user expectations often require careful calibration. The conditions that bring people to infrared therapy, from rheumatoid arthritis to fibromyalgia to sciatica, involve partially overlapping but meaningfully distinct physiological problems.
How infrared reaches pain at the source
The pain-specific effects build on the circulation and tissue-penetration mechanisms already established. What those mechanisms produce, specifically in a pain context, is peripheral vasodilation: blood vessels near the skin and in deeper muscle tissue widen, increasing oxygen-rich blood flow to joints and muscles. That expanded circulation clears metabolic waste, eases local pressure that signals pain, and delivers nutrients that support tissue healing.

Inflammatory joint conditions
For rheumatoid arthritis and osteoarthritis, the evidence is among the strongest in this category. Clinical studies published in PubMed show statistically significant decreases in pain for RA patients, and Mayo Clinic research reports 40% to 60% reductions in pain and stiffness among RA populations in broader studies.
Fibromyalgia
Fibromyalgia may have the most encouraging research in this entire category. Muscle relaxation from deep heat penetration reduces the hypersensitized pain response that characterizes the condition, while endorphin release provides additional relief. A 12-week trial produced pain reductions ranging from 31 to 77% in participants. The lower operating temperatures also make sessions more tolerable for people with fibromyalgia, who are often sensitive to high heat environments.
Sciatica
Sciatica is in a different category. Infrared heat may loosen tight tissues around the sciatic nerve, ease associated muscle spasms, and calm overactive pain receptors. That can translate to meaningful symptom relief. What it cannot do is correct a herniated disc or resolve the structural cause of the compression. Combining infrared sessions with stretching or physical therapy is a more defensible approach than relying on heat alone.
Mental Health, Sleep & Stress Reduction
Sustained infrared exposure shifts the body's autonomic balance away from sympathetic dominance toward parasympathetic activation, the branch of the nervous system governing rest, recovery, and digestion. This shift slows heart rate, reduces muscle tension, and signals the body that no active threat requires a response.
The more consequential mechanism is cortisol modulation: the body's regulation of its primary stress hormone in response to thermal challenge. Core temperature rises during a session; as the body cools afterward, cortisol levels drop. Major institutions like the Mayo Clinic and Cleveland Clinic confirm that infrared sauna use lowers cortisol.
Depression: a consistent direction, an early evidence base
The depression research is interesting, though still preliminary. A 2024 UCSF trial combined infrared whole-body hyperthermia with cognitive behavioral therapy in 16 adults with major depressive disorder. Of the 12 who completed the protocol, 11 no longer met diagnostic criteria after eight weekly sessions. The sample is small, and the combination with CBT makes it impossible to attribute the outcome to heat alone.
Sleep: the timing question
For practical purposes, evening sessions are a reasonable choice for anyone using infrared specifically with sleep in mind. Pairing them with consistent sleep hygiene, rather than relying on the sauna alone, is what the actual evidence supports. Some sources suggest that two to three sessions per week, combined with practices like meditation, may produce more durable results than infrequent use.
Cardiovascular & Circulatory Health
The heart rate and vascular changes that run through stress recovery don't stop there. They accumulate in ways that have drawn genuine scientific attention, and the cardiovascular findings from infrared research are among the more compelling in the field.
The foundational observation came from epidemiologists studying Finnish sauna users. What the data showed restructured how researchers think about passive heat exposure: regular sauna use correlated with reduced cardiovascular events at rates that were comparable to the benefits seen with high cardiorespiratory fitness.
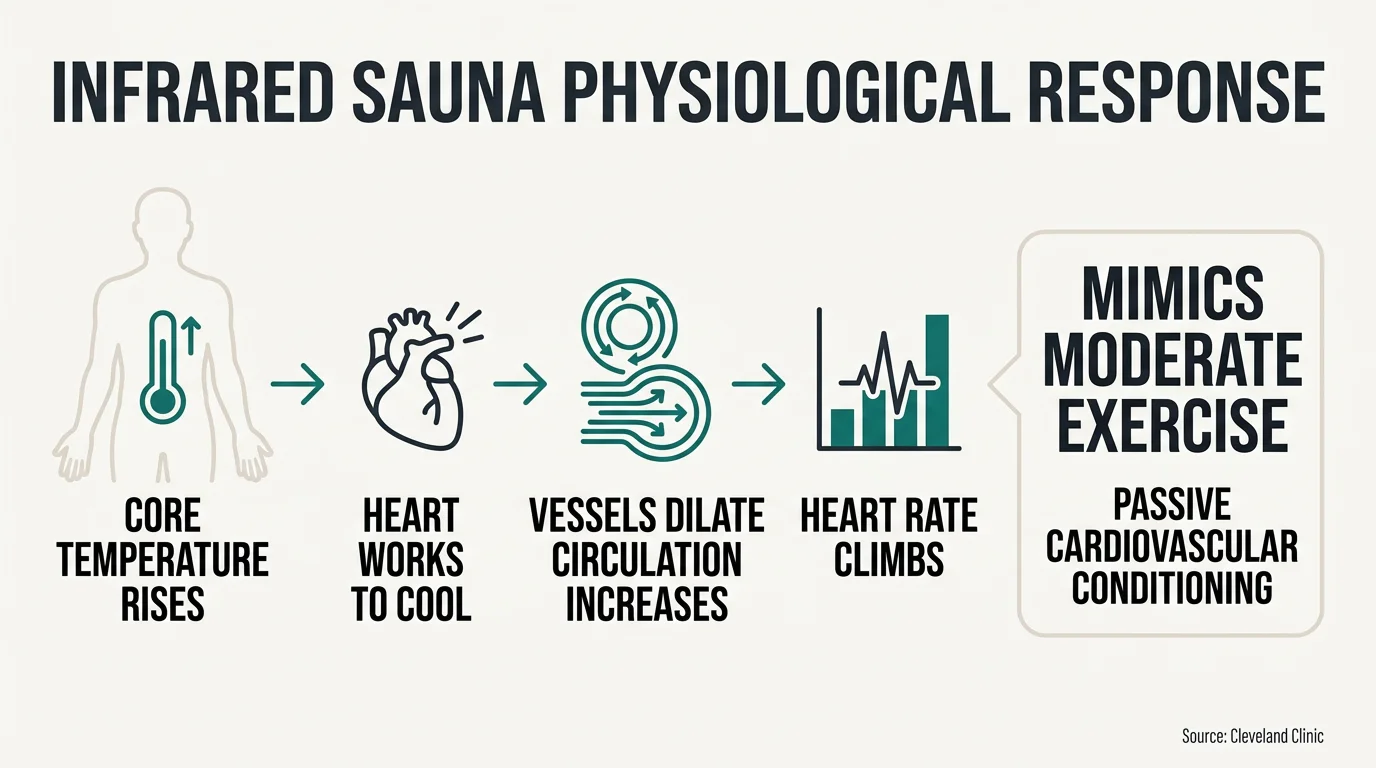
What happens to the heart during a session
During an infrared session, core temperature rises and the body works to cool itself. Heart rate climbs, blood vessels dilate throughout the body, and circulation increases. Cleveland Clinic notes that this physiological response can mimic moderate exercise, which is where the concept of passive cardiovascular conditioning comes in.
Endothelial function: the vessel responsiveness question
Repeated infrared exposure appears to improve endothelial function, which is the ability of blood vessel walls to dilate and constrict appropriately in response to demand. Research published in cardiology-focused literature, including findings reviewed in PMC, suggests these vascular improvements are one of the more biologically plausible pathways through which regular sauna use may support cardiovascular health over time.
Cholesterol: real but indirect
The cholesterol picture is modest. The collective physiological effects of regular sessions — elevated heart rate, improved circulation, vessel dilation — appear to support better lipid profiles over time, per PubMed research. Preliminary support exists, though the evidence is still developing and the effect size is probably modest. Cholesterol levels from beneficial sessions tend to drift back toward baseline after discontinuation. Infrared is not a cholesterol treatment, and positioning it as one overstates the current evidence.
Where caution is warranted
Vasodilation creates specific contraindication concerns. Varicose veins experience increased venous pooling in compromised vessels with heat, potentially worsening rather than improving the condition. Lymphedema involves fluid movement that differs from therapeutic drainage and may worsen swelling. Both warrant physician conversations before any sauna application.
Healthline identifies hypotension as a risk factor, and both Cleveland Clinic and Mayo Clinic advise medical consultation before sessions for anyone with existing cardiovascular conditions. The thermal load that produces conditioning benefits in healthy users can stress compromised systems in ways that require individualized assessment.
Respiratory & Immune System Support
Start with what has real mechanistic support. Infrared heat increases local circulation in the upper respiratory tract and helps drive mucociliary clearance — the process by which cilia sweep mucus and particles outward. Improved clearance eases congestion. This explains why infrared provides temporary symptom relief for sinus congestion in otherwise healthy individuals. Warmth also relaxes bronchial muscles and may loosen mucus, which explains why some asthma or bronchitis sufferers report easier breathing afterward. A study published in PubMed found improvements in forced vital capacity in patients with obstructive pulmonary disease and observed no bronchoconstriction during sessions — an encouraging signal. Mayo Clinic notes, however, that large clinical asthma trials are still lacking, and individual response varies considerably: heat that helps one person's breathing can trigger bronchospasm in another. Medical guidance before using infrared with any respiratory condition remains mandatory.
The immune system: a real mechanism, a modest effect
Cleveland Clinic acknowledges that infrared saunas may help by mimicking a mild fever and enhancing immune responses. Rising core temperature activates heat shock proteins — cellular stress-response molecules that are part of the protective machinery of an actual fever. Far infrared exposure also appears to stimulate white blood cell production and antibody release, according to WebMD, and some epidemiological data connects frequent sauna use to decreased respiratory viral infection incidence. These are genuine signals. What they are not: evidence that infrared kills viruses inside the body. Laboratory virus deactivation requires temperatures of around 65°C or higher, often combined with UV. Infrared sessions bring core temperature to roughly 102°F (39°C), per Cleveland Clinic. That gap is substantial, and sauna heat destroying active infection at the tissue level is not evidence-supported.
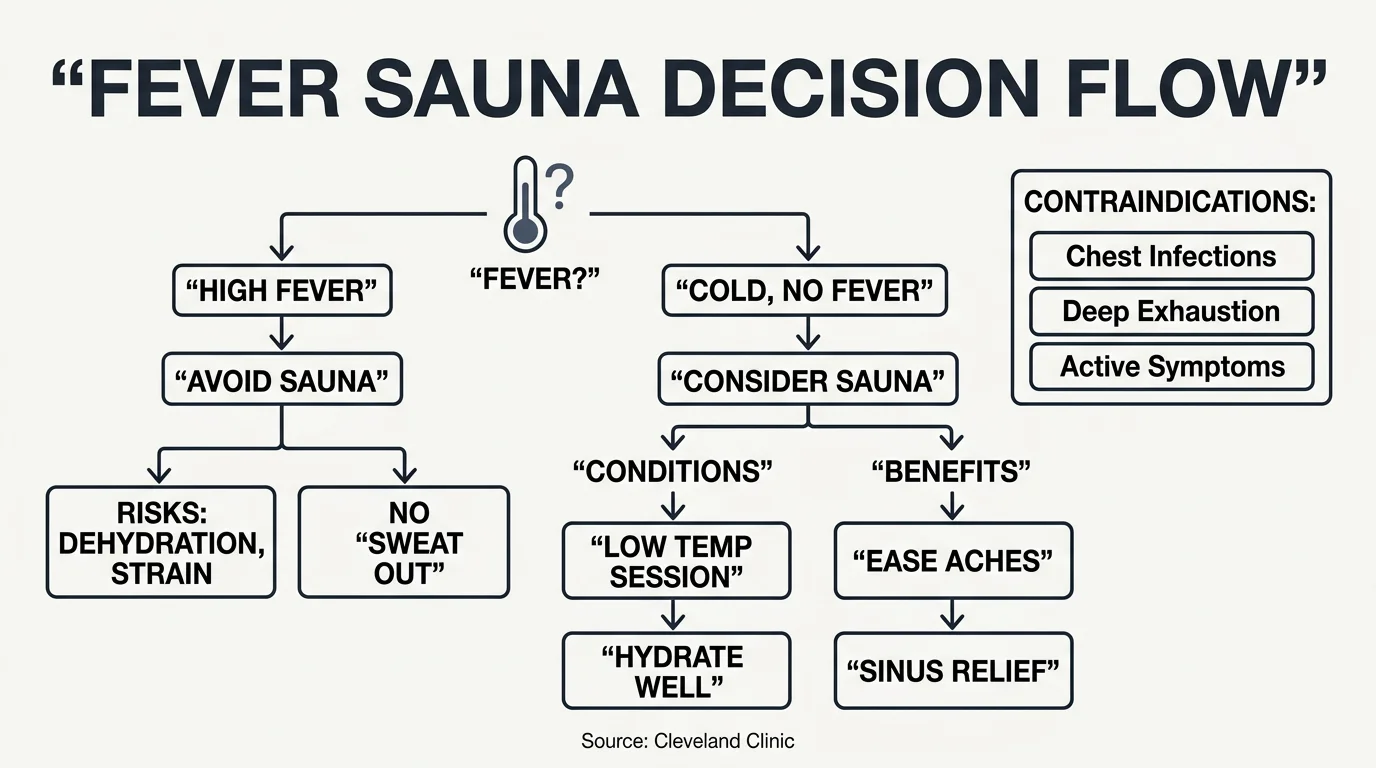
When you're already sick: the fever question
Using infrared during active illness requires careful distinction. For mild cold symptoms without fever, some sources suggest brief, lower-temperature sessions may ease body aches and sinus pressure, provided thorough hydration before, during, and after. Above a 100.4°F (38°C) fever, infrared should be avoided. Adding external heat to an already-febrile state risks dehydration and cardiovascular strain; attempting to "sweat out" an infection accelerates dangerous fluid loss. Chest infections, profound exhaustion, and active systemic symptoms are contraindications, not treatment opportunities. Cleveland Clinic confirms there are no substantial clinical trials supporting infrared as a cold cure, and cold symptom relief evidence remains preliminary.
COVID: a context-dependent answer
Acute illness is a contraindication by the same logic that applies to any active systemic infection. During post-illness recovery, the documented muscle aches, fatigue, and autonomic effects of recovery seem potentially supportive as a complement to rest. Long COVID has drawn genuine clinical interest, but no controlled evidence exists currently, and anecdotal reports are not appropriate as clinical guidance. For healthy adults using infrared regularly, modest cumulative support for innate immune function is the most defensible framing — not acute intervention.
Detoxification & Weight Management
Sweat is not urine. That single biological fact quietly dismantles a significant portion of the infrared detox canon. Sweat's actual job is thermoregulation. That it also carries trace amounts of certain compounds out of the body is real, but it is a secondary effect. The liver and kidneys are the primary detoxification organs, continuously processing metabolic waste at volumes that exceed anything a sauna session contributes to.
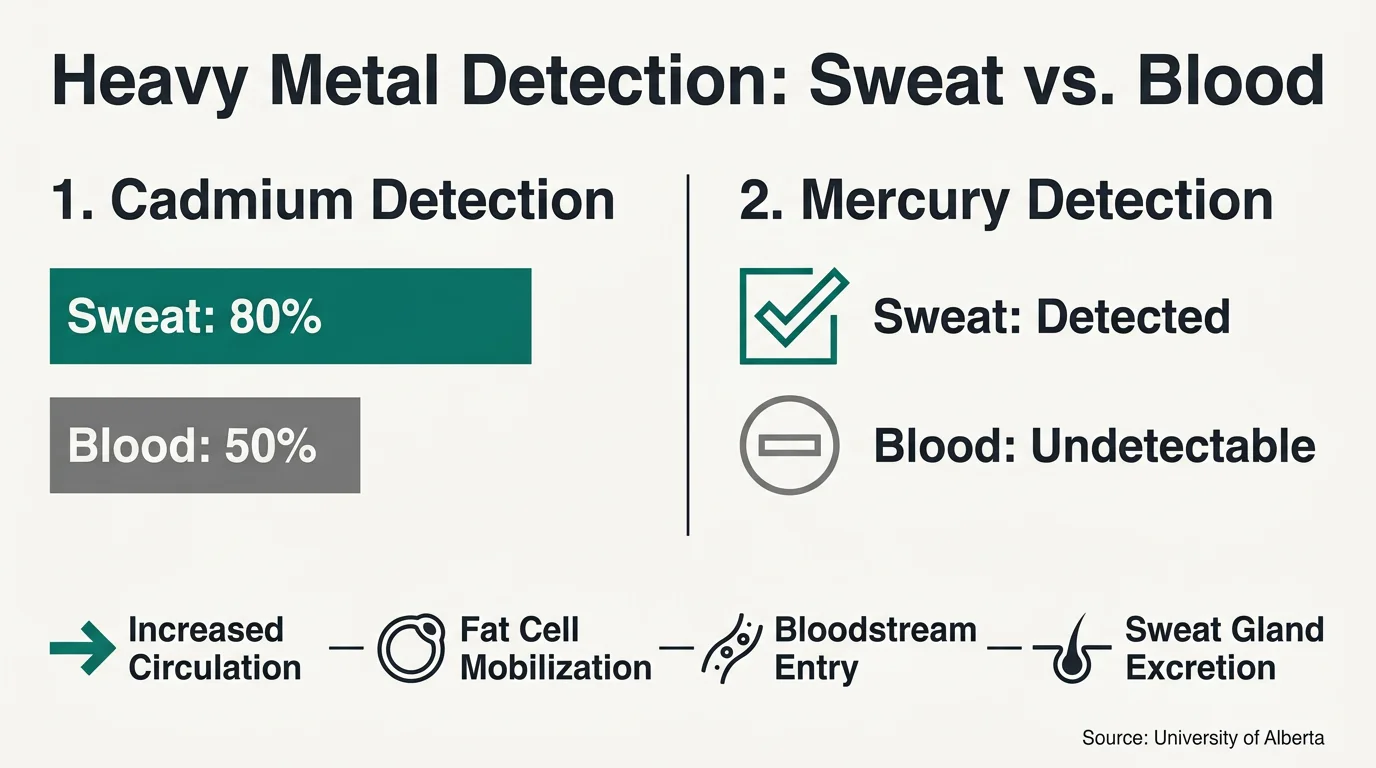
What sweat does contain, in measurable amounts, is a range of exogenous compounds, including certain heavy metals. Research from a University of Alberta study found that sweat was more effective at eliminating some heavy metals than blood or urine alone. Cadmium appeared in roughly 80% of participants' sweat while blood tests detected it in only 50%. Mercury showed up in sweat even for participants where blood tests came back undetectable. These are genuinely intriguing findings. Toxicants including lead and cadmium stored in fat cells may be mobilized by infrared heat's circulation and tissue temperature effects, creating sweat gland pathways. However, the clinical significance for most healthy individuals remains unclear — quantities eliminated per session are modest relative to what the liver and kidneys process continuously, and PMC research is clear that infrared should not constitute primary treatment for documented heavy metal toxicity.
Infrared effects on the lymphatic system
Lymphatic flow enhancement works differently. The lymphatic system has no pump of its own — it relies on muscle action, breathing, and circulation shifts to keep fluid moving. When vasodilation increases circulation during an infrared session, that circulatory activity provides a secondary stimulus to lymphatic flow. Warmer temperatures appear to boost lymph fluid movement, which may help reduce temporary bloating or puffiness. Cleveland Clinic confirms water retention benefits are short-term, and infrared does not address the root causes of chronic retention. These are real and useful effects — they just should not be conflated with clinical lymphatic therapy.
Practical framing
Infrared-induced sweating offers supplemental rather than primary metabolic support. The vascular activity driving cardiovascular and pain benefits simultaneously helps clear inflammatory byproducts and supports the body's waste-removal networks in biologically coherent, if non-transformative, ways. One practical consideration the detox conversation frequently overlooks: sweating eliminates trace minerals alongside waste, which means post-session electrolyte replacement matters, per PMC research. Hydration alone may not fully replace what's lost in heavy sweat sessions. Pre-, during-, and post-session hydration is baseline guidance across Mayo Clinic and PMC sources, and it becomes more important — not less — when sessions are framed around detoxification.
Weight Loss Strategies & Calorie Burning
The calorie expenditure is real. The body expends energy to cool itself, driving an elevated heart rate and triggering thermoregulatory effort that burns calories. Estimates land in the range of 200 to 600 calories for a 30-minute session. None of these figures are guarantees, and they come primarily from non-Tier-1 sources, so they are better understood as reasonable estimates than precise clinical measurements. Body weight, session temperature, duration, and individual baseline metabolism all shift the numbers considerably.
What the scale shows afterward is not what you think
Interpretation matters here. Post-session immediate weight loss partly reflects sweat-related water weight, which reverses with rehydration. A PMC body mass study attributed post-sauna reductions primarily to water loss rather than fat. This is the water-versus-fat-loss distinction that marketing habitually blurs: a lighter number on the scale after a session largely indicates fluid shifts, not changes in adipose tissue.
More relevant is what happens to metabolic rate after sessions end. Some evidence suggests infrared use produces elevated basal metabolic rates afterward, meaning the body continues burning calories at a higher rate beyond the session itself. Cortisol modulation — documented in the mental health section — carries secondary relevance: reduced cortisol associates with conditions less favorable for fat storage, though this pathway's direct weight-loss contribution has not received controlled trial confirmation. Mayo Clinic does not specifically endorse infrared saunas for fat loss, which is itself informative. Weight-loss assertions fall into the evidence tier where gaps between independent research and marketing are most pronounced.
The Binghamton study: what it actually shows
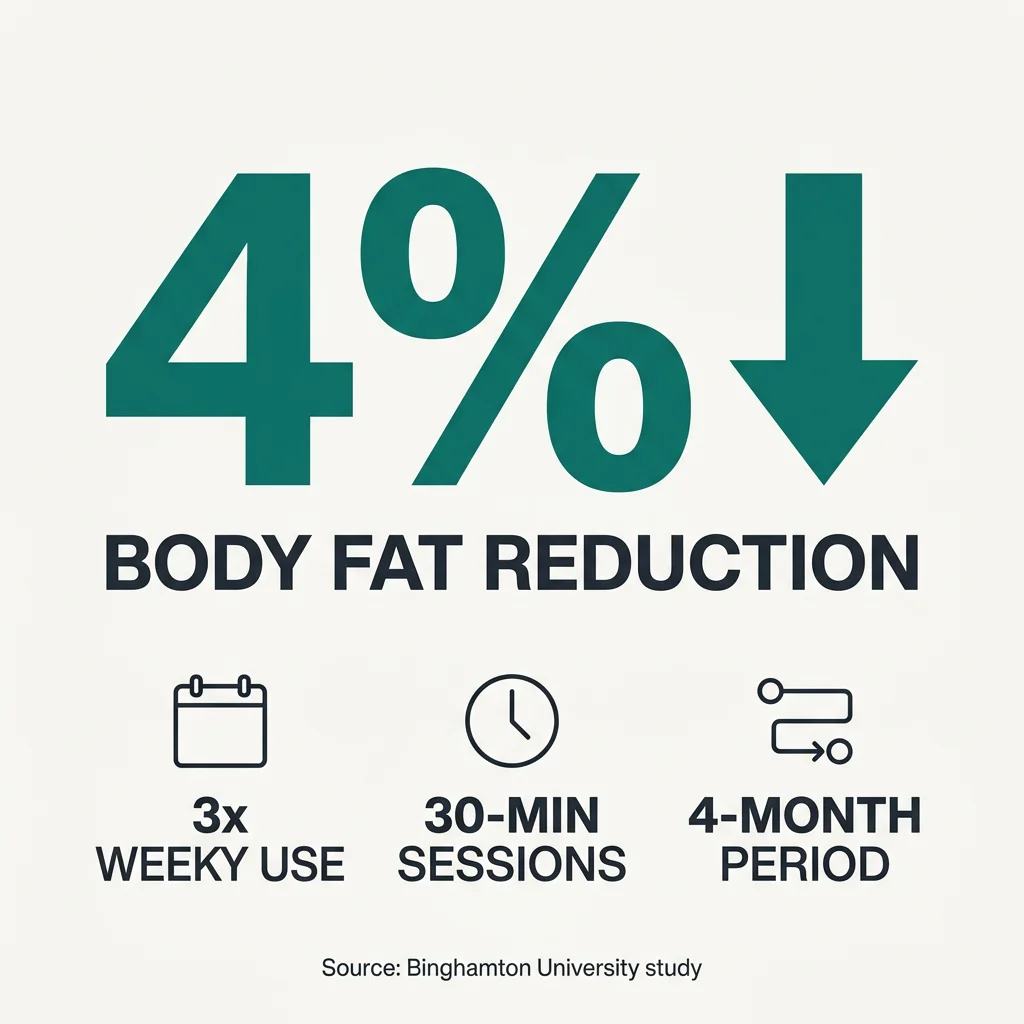
In a Binghamton University study, participants using an infrared sauna three times weekly for 30-minute sessions over four months showed an average 4% reduction in body fat without changes to diet or exercise. This 4% figure is the most specific available clinical data point. It represents genuine findings worth noting, with important context: the study involved specific sauna models, sample sizes were modest, and independent replication has not broadly occurred. Mayo Clinic's consistent caution about study size and the need for larger trials applies directly here.
How to use sessions strategically
For weight management purposes, the most accurate framing treats infrared as a supplemental tool within a broader strategy, not a primary intervention. Mayo Clinic's recommendation pairs sauna use with diet and exercise for users focused on weight goals. Sessions of 30 to 45 minutes at three to five times weekly represent the ranges appearing in more credible outcome data. Consistency outperforms session intensity. Infrared saunas burn calories and modestly contribute to weight management efforts alongside diet and exercise. They cannot replace that effort, and frustration from abandoning them usually traces to treating a supplemental tool as a primary one.
Benefits of Infrared Sauna Blankets
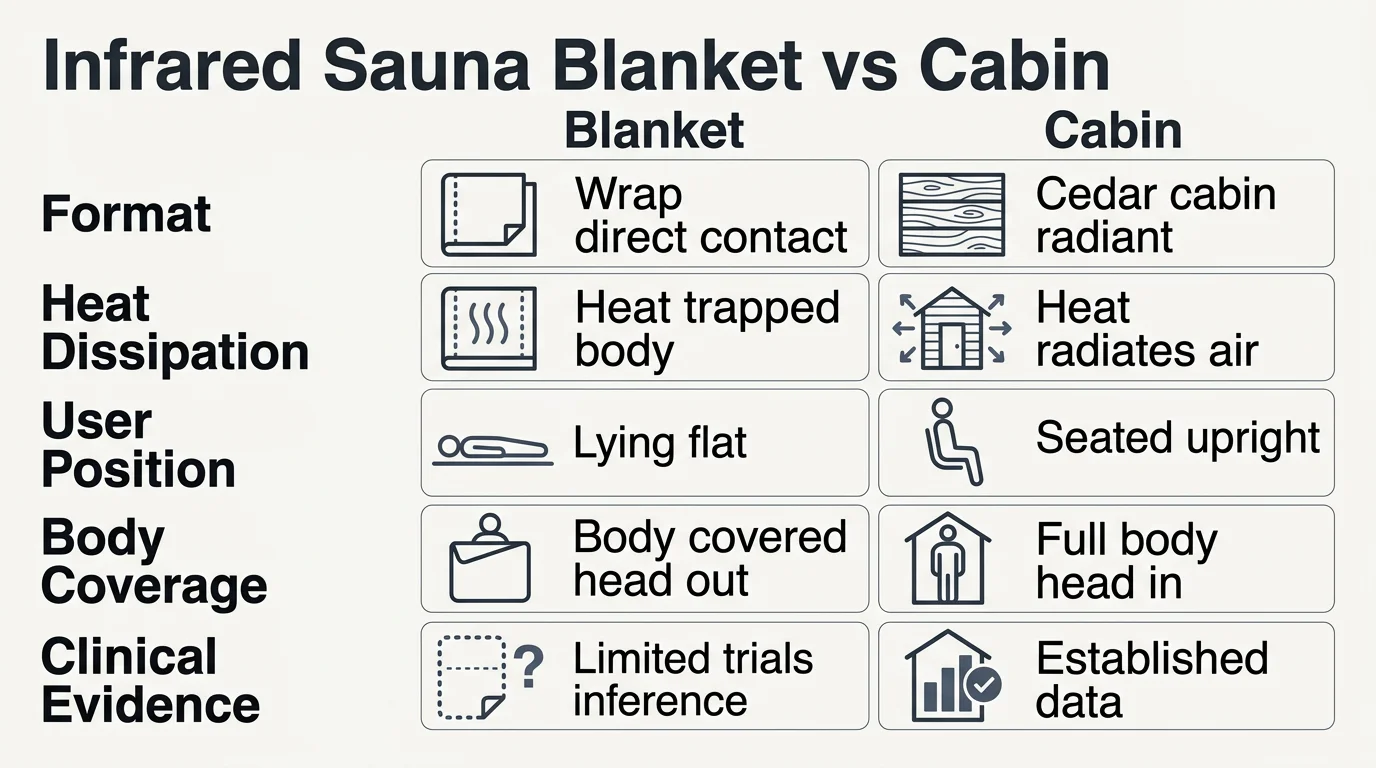
Infrared benefits depend on wavelength absorption and tissue response rather than the structure of the unit. Blankets emit radiation in the far-infrared range, and because they sit in direct contact with the body, penetration depth is physiologically comparable to cabin units. Skin circulation, muscle relaxation, cortisol modulation, and modest metabolic activity all follow the same underlying mechanics regardless of whether you're upright or reclined. Research published in PMC indicates that infrared sauna blankets mimic many of the effects produced by traditional cabin formats.
Practical temperature and hydration considerations
In a cabin, excess heat radiates into the surrounding air. A blanket wraps heat around the body, dramatically reducing its ability to escape. Skin-surface temperatures build faster and climb higher at the same thermostat setting. Healthline recommends keeping blanket temperatures within the 140°F to 160°F range. Users who max the settings typically feel overheated quickly, shortening sessions before meaningful physiological benefits accumulate. Dehydration risk follows the same logic — sweat has a diminished evaporation surface when wrapped, meaning fluid loss may exceed what you're aware of. The hydration guidance that applies to cabin use applies with equal or greater force here.
Coverage and positioning considerations
Blankets cover the body while leaving the head outside the enclosure. For most of the benefits discussed in this article, this is a minor limitation: cardiovascular loading, peripheral vasodilation, muscle relaxation, and autonomic shifts respond primarily to core body heating rather than facial temperature. The reclined position does alter cardiovascular loading compared to seated cabin use — horizontal positioning reduces the gravitational demands on the heart compared to vertical — though whether this meaningfully changes cardiovascular outcomes remains unestablished in current blanket-specific research.
Evidence quality and research availability
Clinical infrared blanket-specific research remains limited. The cardiovascular, musculoskeletal, and autonomic data referenced throughout this article comes almost exclusively from cabin-format trials. Direct blanket-specific clinical evidence is thin. The equivalence case rests on mechanism inference: comparable wavelengths, penetration depths, and tissue responses should produce identical physiological cascades. That reasoning is biologically coherent but lacks the broad controlled trial testing that cabin formats have accumulated. For individuals evaluating blankets as a cost-efficient, space-efficient entry point into infrared therapy, the core benefits remain accessible. Conservative session management applies: respect the temperature ceiling, hydrate consistently, and acknowledge that reduced heat dissipation means safer duration baselines differ from cabin settings. Anyone with cardiovascular or other contraindications should consult a physician before blanket use — the thermal stimulus guidance applies regardless of format.
Timeline For Experiencing Results
The timeline for results depends on which benefit you are pursuing, because acute effects and adaptive effects operate on fundamentally different clocks.
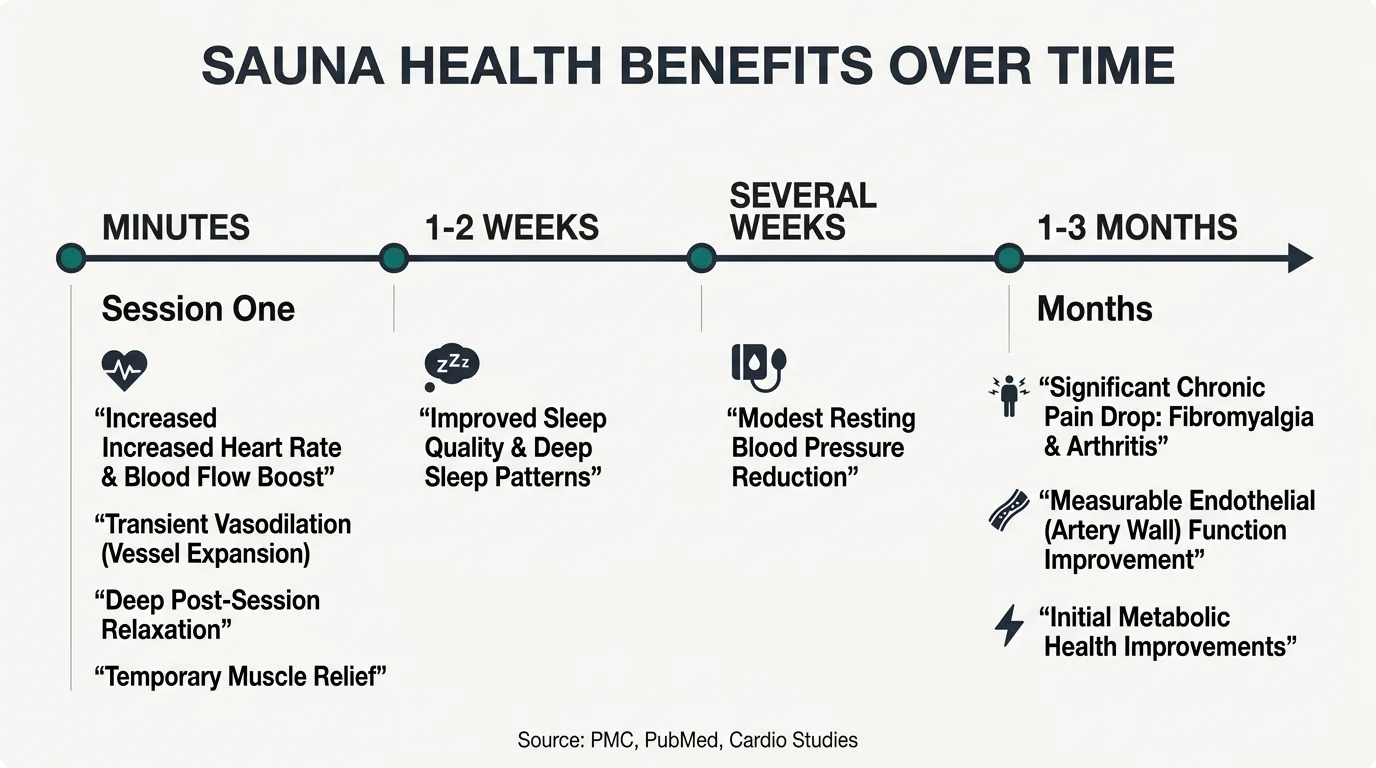
Acute benefits (single session effects)
Acute benefits are available from the first session. Cardiovascular responses begin within minutes: heart rate rises, peripheral vasodilation occurs, and circulation increases measurably. Post-session relaxation — the parasympathetic shift documented in the mental health and cardiovascular sections — is immediately accessible. Muscle tension reduction and temporary skin circulation improvement fall into the same category. These are real effects, though transient. They normalize as the heating ends.
Adaptive benefits (cumulative effects)
Adaptive benefits are fundamentally different. They require repeated exposure because the body needs consistent signals before implementing lasting structural or functional changes. Sleep quality improvements appear to develop within one to two weeks of regular use across multiple sources, rather than from individual sessions. Modest blood pressure reductions, documented in PMC cardiovascular research, emerge through regular weekly sessions spanning several weeks. Skin texture improvements tied to fibroblast activity require consistent application because collagen remodeling proceeds slowly. Meaningful chronic pain score reductions for fibromyalgia and arthritis typically fall within one-to-three-month sustained-use windows, consistent with PMC chronic pain and PubMed fibromyalgia trial findings. Cardiovascular markers including endothelial function improvements generally require one-to-three months of regular sessions.
The adaptation threshold concept
An underlying principle connects all of this: an adaptation threshold — a consistent frequency and duration requirement before cumulative physiological change initiates. Both Mayo Clinic and Cleveland Clinic acknowledge stronger evidence for consistent versus isolated use. That carries practical implications. Intermittent use with week-plus gaps largely prevents adaptive benefit accumulation. The body responds to consistent thermal signals, not occasional ones. Frequency guidance in more credible outcome data emphasizes three to five weekly sessions, with individual sessions of 15 to 30 minutes for beginners expanding as tolerance develops.
Consistency, not session intensity, is the variable that separates people who experience compounding benefit from those who report that infrared saunas didn't work for them.
Specific Condition Efficacy
For people researching infrared sauna use alongside a serious diagnosis, the most useful thing any guide can do is draw a clear line between where evidence exists and where it runs out. The line sits in different places for different conditions. More serious conditions require higher evidence standards before use recommendations, and physician consultation shifts from advisable to essential.
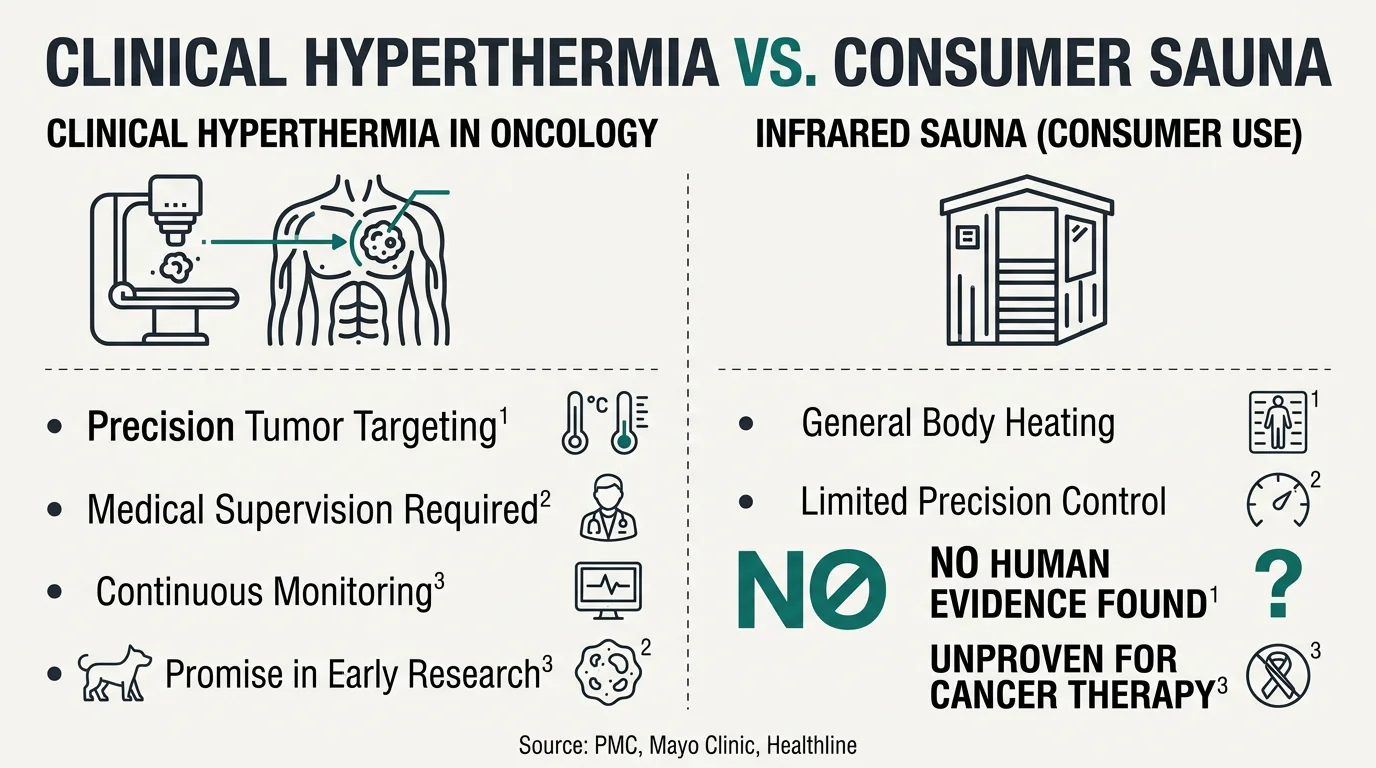
Cancer
Clinical hyperthermia, as used in oncology, involves raising tissue temperatures in precise, targeted zones to sensitize cancer cells to chemotherapy or radiation. It is a controlled medical procedure with calibrated equipment and monitoring throughout. PMC-reviewed research confirms preliminary promise in animal studies and cell line work, but no conclusive proof of efficacy exists in humans for sauna-based cancer therapy. Consumer sauna sessions bring core temperature to roughly 102°F (39°C) — clinical hyperthermia targets specific tissues at precision-calibrated temperatures that home saunas cannot achieve. Anyone in active cancer treatment must consult their oncologist before using infrared in any format. This is non-negotiable.
Multiple Sclerosis
MS presents a straightforward concern. Heat exacerbates MS symptoms for many individuals, and symptoms can temporarily worsen with body temperature increases. Published research specifically studying infrared for MS is essentially absent, and the potential for symptom flare makes physician consultation mandatory. This is a condition where conservative approaches warrant strong priority.
Lupus and Autoimmune Conditions
Evidence supporting benefits for autoimmune diseases broadly comes primarily from small studies. The immune-modulating effects that help rheumatoid arthritis cannot be assumed to translate predictably to lupus. Lupus-specific complications matter practically: photosensitivity in some individuals, heat intolerance, and specific lupus medications can all interact adversely with heat. Sessions should stop if flares occur. Medical consultation before starting is not optional.
Lyme Disease
Infrared appears in integrative discussions as a potential tool for reducing herxheimer reactions — the temporary symptom worsening that can follow treatment. This application's evidence remains anecdotal. Active Lyme frequently involves cardiovascular compromise and systemic impairment, making the thermal load of a sauna session a meaningful consideration. Physician oversight before infrared use is necessary here.
Menopause
This is a more plausible application category. Heat may paradoxically decrease vasomotor symptoms including hot flashes via autonomic regulation, and the cortisol-modulating effects documented in the mental health section apply directly to the hormonal stress context of perimenopause and menopause. The mechanistic reasoning is coherent, though large controlled infrared-and-menopause trials remain limited. Risk profiles for otherwise healthy individuals are favorable, and the evidence-to-risk ratio is relatively positive here absent cardiovascular contraindications.
Other Conditions
Lipedema has drawn patient community interest, though peer-reviewed infrared-specific research for this population essentially does not exist. The lymphatic flow advantages discussed earlier are biologically plausible but not clinically established for lipedema specifically. Hangover use carries minimal risk in generally healthy individuals, with limited effects; the primary concern is cardiovascular strain on a dehydrated system, and the standard hydration guidance applies with greater force from a fluid-depleted baseline.
Synthesis and Practical Conclusions
The preceding sections describe a technology with genuine but bounded effects. Infrared produces measurable physiological changes with real condition-specific benefits. It also exhausts its explanatory power well before some of the more ambitious claims made about it.
The pattern is consistent across every domain. Where a mechanism logically connects to an outcome and research substantiates that logic, the evidence is encouraging. Cardiovascular conditioning, blood pressure support, pain relief for inflammatory joint conditions and fibromyalgia, skin maintenance, and cortisol modulation all have coherent biological backing. Where claimed benefits outrun the mechanisms or independent research hasn't matched the marketing, the current evidence is insufficient. Primary weight loss outcomes, cancer intervention, and broad detoxification claims fall into that second category.
Several threads run through every section and are worth pulling together. The adaptation threshold matters more than any single session. Cardiovascular improvements, sleep benefits, chronic pain score reductions, and immune resilience all require consistent repeated sessions over weeks to months before they become measurable. Showing up three to four times weekly for several months reflects the actual study structures that identified meaningful findings — not marketing framing.
Condition-severity risk stratification applies globally. For generally healthy individuals, infrared shows a favorable safety profile at typical operating temperatures. For anyone managing a serious diagnosis — cardiovascular disease, autoimmune conditions, cancer, or neurological illness — physician consultation is a non-negotiable requirement. The thermal load that produces conditioning benefits in healthy users interacts with disease activity, medications, and treatment protocols in ways that require individual medical assessment.
Blankets and cabins share the same core mechanisms. The evidence for one largely supports the other. Practical session-management differences exist, but the fundamental biology does not change based on the hardware.
The appropriate framework positions infrared as a well-characterized complementary tool. Not a medical treatment. Not a shortcut. Not a cure. A tool that, with consistent use and appropriate medical guidance where circumstances require it, can meaningfully contribute to recovery, resilience, and quality of life. For the right person, with realistic expectations, consistent application, and any needed physician input, the contribution is meaningful. The evidence supports saying that clearly — and it equally supports being honest about where that evidence ends.